

Much like 2021, the first UCSF Grand Rounds of this year began grimly. Amid the bloody backdrop of insurrection in our nation’s capital, over 4,000 daily Covid-19 deaths in the United States, and a shaky national vaccine rollout, a new threat has emerged, said UCSF Medical Department Chair and Grand Rounds moderator Dr. Bob Wachter.
“We thought we were running a race against a virus that we didn’t know a year ago, but we’d come to understand—and mostly hate—over the past year. And it now seems to have morphed into a few different versions of itself, some of which are better at some of the things that it does, including infectivity and maybe even evading the vaccine to some extent,” Wachter said. “So the stakes have been raised and the need for speed has grown even more in the last couple of months.”
UCSF vaccine rollout
UCSF Health Chief Pharmacy Executive Desi Kotis and Chief Faculty Practice Officer Susan Smith returned to Grand Rounds with updates regarding vaccine distribution at UCSF, which has administered over 20,000 doses as of Thursday morning. Though UCSF is still mostly on first doses, Smith said that they are starting to increase the administration of second doses, for those who got their first, on Jan. 6.
Of the 23,218 people in Phase 1A at UCSF, 99 percent have been offered the vaccine, 82 percent have consented to receive it, and 77 percent have received their first dose.

Kotis said that they have not had to administer any epinephrine shots during the rollout, but have given antihistamines such as Benadryl “a couple of times” and observed some dizziness. Smith said, anecdotally, she has heard of more muscle soreness and fever associated with the second dose.
Though some individuals have not consented to the vaccine, Smith believes this may be due to digital literacy problems (as indicated by the gap in activity on MyChart, which is UCSF’s online patient portal) and language barriers, as opposed to vaccine hesitancy. However, she noted differences in sign-ups among different races and ethnicities, stating that “we’re going to take a deeper dive in conjunction with some of our diversity, equity and inclusion people at UCSF to understand that better and see if there’s mitigations that we can help with.”
UCSF is working toward a more open-access web format as it expands access to elderly patients, beginning with those who are older than 75 and later expanding to patients 65 years and up.
Though “the vaccine is not coming by any way, shape or form through traditional supply chain for drugs,” Kotis said, 80 to 85 percent of UCSF’s first doses have been administered or are reserved for next-day appointments. Wachter compared this to the national average of 30 percent, and California’s average of 25.
“We are doing amazingly well, in terms of sort of getting it from the freezer to people’s arms,” he said.
Cautious optimism for herd immunity
Paul Offit, director of the Vaccine Education Center at Philadelphia Children’s Hospital and one of the “foremost experts on vaccines in the world,” according to Wachter, next presented a dose of optimism. The efficacy of the currently approved vaccines and several other vaccines that are around the corner are good signs, he said.
Offit, who is on the Food and Drug Administration’s Vaccine Advisory Committee, believes the FDA will be hearing about either the AstraZeneca or Johnson & Johnson vaccine in February, with the goal to get them out in March. Two more vaccines from Novartis and Sanofi/GSK will hopefully be released in April, he said.
Offit is also optimistic, because he believes the number of people in the U.S. who have already been infected with covid is closer to 65 or 70 million—as opposed to the official number of 23 million—because of several recent studies indicating that the official number “is probably off by a factor of three to four,” he said. If true, this would mean that 20 percent of the nation’s population already has some immunity to the virus.
Using a formula by epidemiologist Paul Fine to determine herd immunity threshold, he estimates that it could be achieved with a mere 60 percent percent of the population vaccinated and/or previously infected with the virus. This could be achieved by vaccinating one to 1.5 million people per day.
The barrier to such a goal (as the U.S. is currently vaccinating about 500,000 people each day) is that “we’re trying to create a public health infrastructure that doesn’t currently exist,” Moffit said.
That is evident in San Francisco, where the rollout has been excruciatingly slow.
Wachter seemed hesitant to accept 60 percent, noting that Dr. Anthony Fauci predicted closer to 80 percent, especially considering that there will be crossover between people who have already been infected and those who are receiving the vaccine.
As for mutations, Offit said the question is whether covid will behave like influenza, which requires new vaccines every year, or if it will be like the measles, which has required only one since the vaccine was developed in 1963. Covid, he said, “will probably be somewhere in between.”
A tale of three variants
The effects of Offit’s optimism waned throughout Dr. Charles Chiu’s presentation. The professor of medicine at UCSF’s Division of Infectious Diseases discussed three potentially dangerous variants to the SARS-CoV-2 virus, the virus that causes Covid-19, that have emerged.
The coronavirus is unique compared to other single-strand RNA viruses, due to an error-coding protein that actually corrects for mutations in the viral genome, meaning it mutates much slower than other RNA viruses.
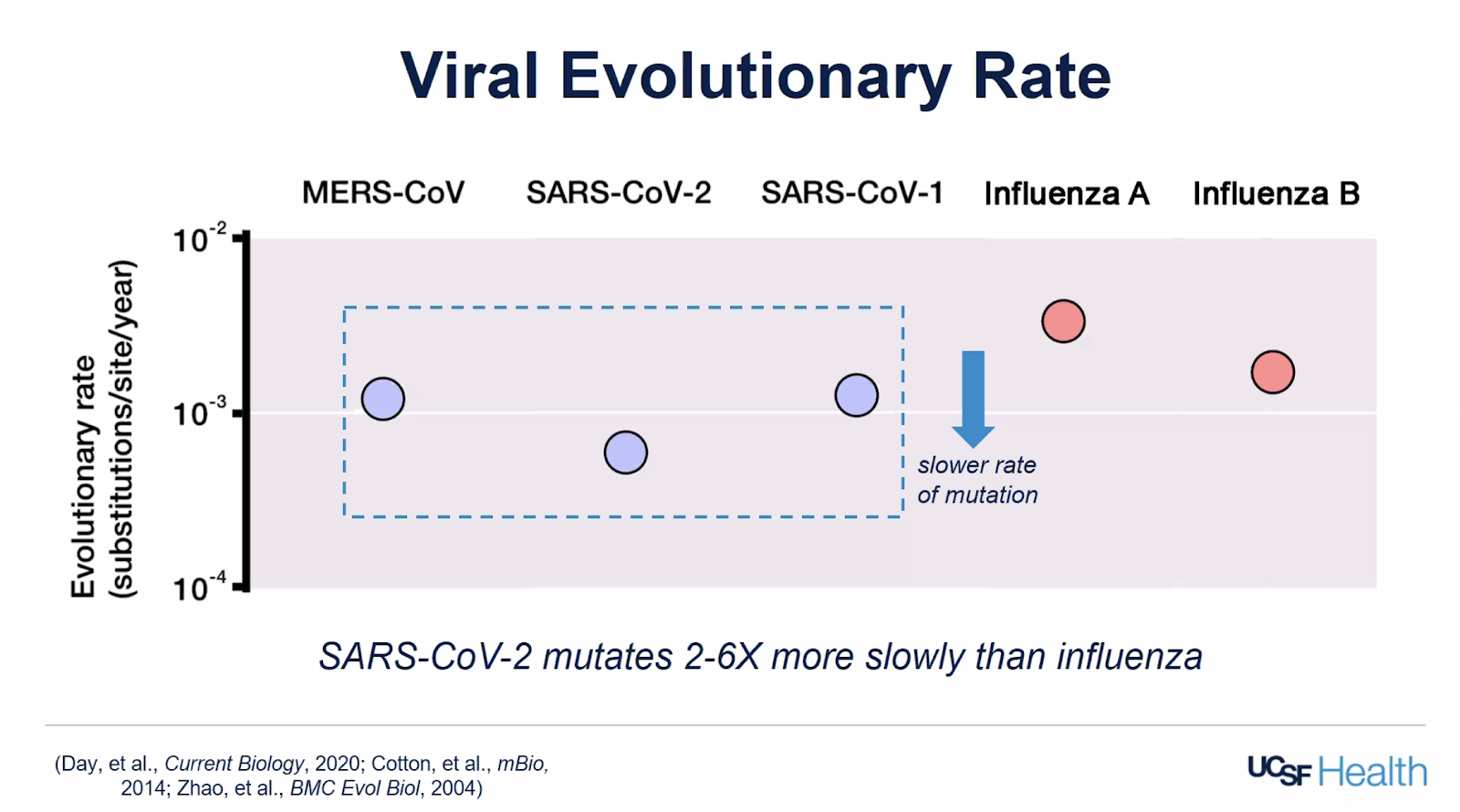
However, this hasn’t stopped mutations altogether.
One of the first significant mutations that arose back in March is the D614G spike protein mutation. This occurs in the protein that allows the virus to fuse with and infect our body’s cells, and is now present in 99 percent of all circulating viruses. One reason why researchers postulated this mutation’s rapid spread is that it has been shown to increase infectivity in cell culture and replicates better in animal models, Chiu said.
“The take-home message is that we’re really in a race now, and really this only increases our urgency to mass vaccinate the population and protect the population before additional variants may evolve and emerge.”
Charles Chiu
Another variant that has been making headlines is B.1.1.7, also called the United Kingdom variant. This variant emerged in September, is considered “highly transmissible,” and has already spread to 31 countries, including 76 confirmed cases in the United States. While it initially made up five to 10 percent of cases in November in the UK, it now makes up over 60 percent.
What is unusual about this variant is the sheer number of mutations present; while scientists typically observe one to two mutations a month, this variant has 23, despite emerging only in September, Chiu said.
One property of this variant, the deletion of the 6970 nucleotide sequence, “has been useful for us, with respect to being able to identify these mutations,” Chiu said. When testing for the virus, tests often look for the presence of several target genes, one of which is the gene deleted by this mutation. When an individual tests positive for covid but this specific gene is missing, this indicates they have been infected with a variant strain.
Though this strain is more transmissible and thus may warrant greater speed in the vaccination rollout, the “really good news” is that this vaccine appears to neutralize this variant. However, the same cannot be said of the South African variant, which Chiu called “quite worrisome.”
The SA variant includes the E484K mutation, a mutation that can occur on the spike protein and “may potentially enable the virus to evade vaccines or monoclonal antibody therapies [laboratory-produced molecules that fight off the virus],” Chiu said, citing several recent preprint studies. This means that antibodies produced by the body in response to infection or vaccination may not be as effective against viruses with this mutation.
Chiu did specify that this is suggestive data from laboratories, but what is really needed is direct data to answer the question of this mutation’s effect on vaccine efficacy. He suspects that if the mutation does impact an individual’s immune response to the virus, the impact would not be universal across those infected with it. He also said that it is “hopefully going to be a very slight difference and not, say, a significant difference that may, for instance, require a new vaccine,” because vaccines target the entire viral genome.
The SA variant is not present in the U.S. yet, but has been found in 11 countries.
“The take-home message is that we’re really in a race now, and really this only increases our urgency to mass vaccinate the population and protect the population before additional variants may evolve and emerge,” Chiu said.
See our previous Grand Rounds coverage here.
I am 78 and looking hard to get a Covid Vaccine shot. Young lady on channel 2 news at 10pm Sunday on Jan 17 gave the email address to contact you to get on the list. She said it so quickly and I could not get it. Please send me the link to get on your list. I am
quickly available to get the shot. Tested negative last week at Stanford site.
Thank you
Richard Rosencrantz
Thanks for your work summarizing the Grand Rounds while not losing the science, so helpful!